Proctitis vs IBS Symptom Checker
This tool helps identify overlapping symptoms between Proctitis and IBS. Use it to understand shared and unique symptoms, and learn about diagnostic approaches.
Proctitis Symptoms
- Rectal bleeding or bloody mucus
- Frequent urge to defecate with little stool
- Cramping or burning sensation in the lower abdomen
- Feeling of incomplete emptying
- Localized pain in the rectum and perianal area
IBS Symptoms
- Abdominal cramping relieved by bowel movements
- Urgent need to go with gas or mucus
- Bloating and sense of incomplete emptying
- Diarrhea, constipation, or mixed stool patterns
- Diffuse abdominal pain, often lower left quadrant
Overlapping Symptoms
These symptoms occur in both conditions:
- Abdominal cramping
- Urgency to defecate
- Feeling of incomplete emptying
- Mucus in stool
- Bloating
Note: While symptoms may be similar, the underlying causes and diagnostic methods differ significantly.
Key Diagnostic Differences
| Aspect | Proctitis | IBS |
|---|---|---|
| Primary Cause | Inflammation of rectal mucosa | Functional motility disorder |
| Inflammation Markers | Elevated CRP/ESR, visible on endoscopy | Usually normal |
| Pain Location | Lower rectum, perianal region | Diffuse abdominal, often lower left quadrant |
| Stool Consistency | May contain blood or mucus | Diarrhea, constipation, or mixed |
| Diagnostic Test | Colonoscopy / sigmoidoscopy with biopsy | Rome IV symptom criteria |
Important Note: This tool provides educational information only. For accurate diagnosis and treatment, always consult with a healthcare provider. If experiencing persistent or severe symptoms, seek immediate medical attention.
Ever wondered why a flare‑up in the rectum sometimes feels a lot like the cramping you get with IBS? You’re not alone. Many people experience overlapping pain, urgency, and bowel changes, and the medical community is still piecing together how Proctitis and IBS influence each other. This article breaks down what each condition is, where they intersect, and what you can do to feel better.
TL;DR
- Proctitis = inflammation of the rectal lining; IBS = functional disorder causing bowel‑movement irregularities.
- Both can trigger abdominal pain, urgency, and mucus in stool.
- Shared triggers: gut‑microbiome imbalance, stress, and certain infections.
- Diagnosis requires separate tests: proctitis needs visual exams; IBS is diagnosed by symptom criteria.
- Treatment often overlaps: diet changes, probiotics, stress‑reduction, and targeted meds.
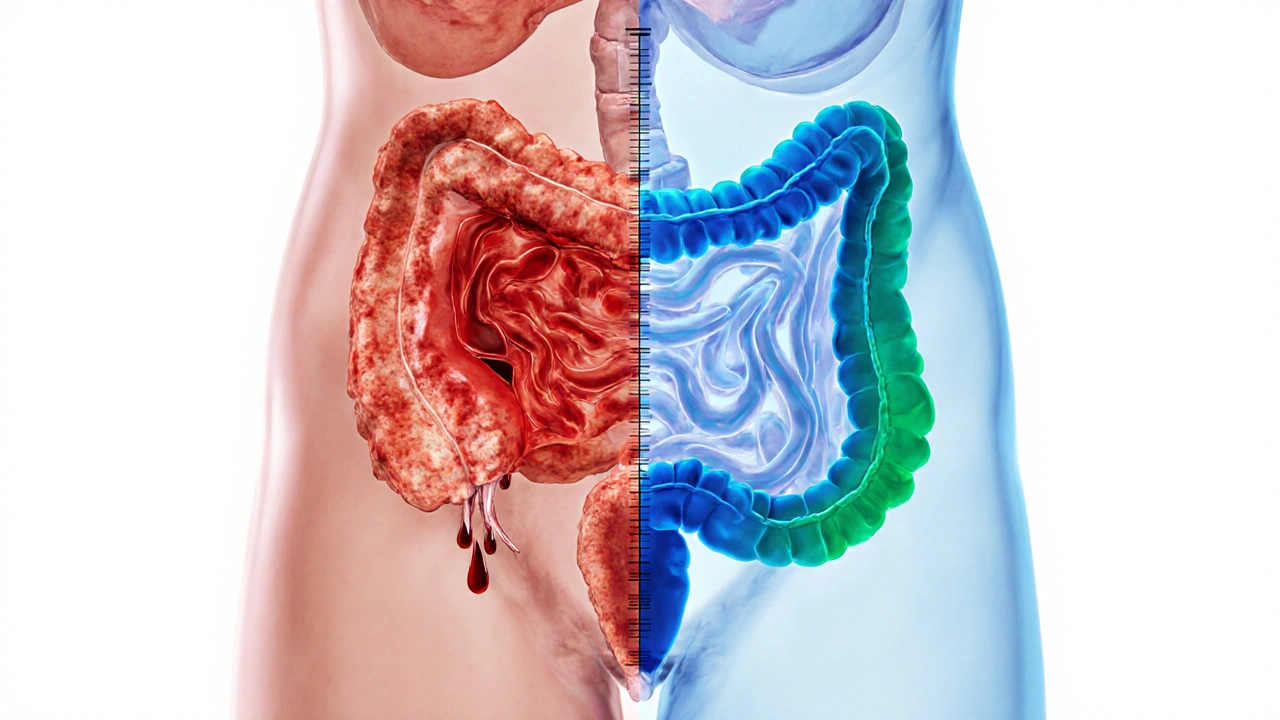
What Is Proctitis?
Proctitis is an inflammation of the lining of the rectum, the final segment of the large intestine that stores stool before evacuation. It can be acute - showing up after an infection or radiation therapy - or chronic, linked to inflammatory bowel disease (IBD) or autoimmune disorders. Common symptoms include:
- Rectal bleeding or bloody mucus
- Frequent urge to defecate, often with little stool
- Cramping or burning sensation in the lower abdomen
- Feeling of incomplete emptying
Because the rectum sits just above the anal canal, proctitis often feels like a sore ankle that won’t quit - tiny, sharp, and localized.
What Is Irritable Bowel Syndrome (IBS)?
Irritable Bowel Syndrome, commonly abbreviated as IBS, is a functional gastrointestinal disorder. Unlike proctitis, IBS does not involve visible inflammation or structural damage. Instead, it reflects abnormal gut motility, heightened pain perception, and often an imbalance in the gut microbiome. The three classic sub‑types are:
- IBS‑D: diarrhea‑predominant
- IBS‑C: constipation‑predominant
- IBS‑M: mixed pattern
Typical IBS symptoms overlap with proctitis, which is why the two are frequently confused:
- Abdominal cramping relieved by bowel movements
- Urgent need to go, sometimes with only gas or mucus
- Bloating and a sense of incomplete emptying
Where the Symptoms Cross: Overlap and Misdiagnosis
Both conditions can produce a “rush to the bathroom” scenario, but the underlying mechanisms differ. The convergence happens through three main pathways:
- Inflammatory spill‑over: Even low‑grade inflammation in the rectum can sensitize nearby nerves, amplifying the pain signals that IBS patients already experience.
- Gut‑microbiome disruption: A study from the European Gastroenterology Society (2023) showed that 38% of patients with chronic proctitis also met RomeIV criteria for IBS, suggesting that dysbiosis may fuel both disorders.
- Stress‑induced motility changes: The brain‑gut axis reacts similarly whether the trigger is inflammation or functional dysregulation, leading to overlapping urgency and stool‑consistency changes.
Because of this overlap, doctors often run a battery of tests to rule out one before confirming the other.

How Doctors Tell Them Apart
Diagnosing proctitis and IBS requires different tools, though some tests serve both purposes.
- Colonoscopy or Flexible sigmoidoscopy: Direct visual inspection reveals inflamed mucosa, ulcerations, or hemorrhage - hallmarks of proctitis. IBS patients usually have a normal‑looking colon.
- Biopsy: Tissue taken during endoscopy can confirm inflammatory cells, ruling out IBD or infection.
- RomeIV criteria: A symptom‑based checklist (recurrent abdominal pain ≥1day/week for the past 3months, associated with defecation changes) is the gold standard for IBS.
- Stool tests: Used to exclude infection (e.g., Clostridioides difficile) that could cause secondary proctitis.
- Blood work: Elevated inflammatory markers (CRP, ESR) might hint at proctitis, while IBS typically shows normal labs.
Managing Both Conditions: Shared and Separate Strategies
Even though the root causes diverge, treatment plans often overlap because the symptom burden is similar.
Dietary Tweaks
- Low‑FODMAP diet: Reduces fermentable carbs that can aggravate IBS; many patients with proctitis also report fewer flare‑ups when they limit high‑sugar foods.
- Fiber balance: Soluble fiber (psyllium) can soothe IBS‑C, while a short course of low‑residue diet eases proctitis during acute inflammation.
Medications
- 5‑ASA suppositories (mesalamine) are frontline for mild‑to‑moderate proctitis, reducing rectal inflammation.
- Antispasmodics (e.g., hyoscine) help IBS cramps by relaxing smooth muscle.
- Probiotics: Strains like Bifidobacterium infantis have evidence for both IBS symptom relief and restoring gut barrier function in proctitis.
- When anxiety drives IBS, low‑dose tricyclic antidepressants can lower pain perception.
Stress‑Management Tools
Because the brain‑gut axis is a two‑way street, mind‑body techniques work for both:
- Mindfulness‑based stress reduction (MBSR) - 8‑week program improves IBS scores by up to 30% (American Journal of Gastroenterology, 2022).
- Biofeedback for pelvic floor dysfunction reduces urgency in proctitis patients who have developed spasm.
When to Choose Targeted Therapy
If symptoms persist despite lifestyle changes, doctors may prescribe:
- Topical steroids (e.g., budesonide) for refractory proctitis.
- Rifaximin or neomycin for IBS‑D with suspected small‑intestinal bacterial overgrowth (SIBO).
Quick Reference: Proctitis vs. IBS
| Aspect | Proctitis | Irritable Bowel Syndrome |
|---|---|---|
| Primary cause | Inflammation of rectal mucosa | Functional motility disorder |
| Inflammation markers | Elevated CRP/ESR, visible on endoscopy | Usually normal |
| Typical pain location | Lower rectum, perianal region | Diffuse abdominal, often lower left quadrant |
| Stool consistency | May contain blood or mucus | Diarrhea, constipation, or mixed |
| Diagnostic test | Colonoscopy / sigmoidoscopy with biopsy | Rome IV symptom criteria |
| First‑line treatment | 5‑ASA suppositories, steroids | Dietary changes, antispasmodics |
When to Call Your Doctor
Both conditions can be managed, but certain red flags demand prompt medical attention:
- Sudden, severe rectal bleeding
- Unexplained weight loss or anemia
- Persistent fever or night sweats
- Symptoms lasting longer than 3months despite treatment
If you notice any of these, schedule an appointment ASAP - early diagnosis prevents complications such as strictures in proctitis or chronic pain cycles in IBS.
Living with Both: A Practical Checklist
- Track symptoms daily (pain level, stool type, urgency) in a simple app or notebook.
- Identify trigger foods - keep a 2‑week elimination log.
- Maintain a regular exercise routine; even a 20‑minute walk reduces stress hormones.
- Schedule routine follow‑ups: endoscopy every 1‑2years if you have chronic proctitis; reassess IBS criteria annually.
- Stay up‑to‑date on vaccinations (e.g., flu, COVID‑19) - infections can spark proctitis flare‑ups.

Frequently Asked Questions
Can IBS cause proctitis?
IBS itself doesn’t cause inflammation, but chronic bowel irritation can weaken the rectal lining, making it more susceptible to secondary inflammation. In practice, a small percentage of IBS patients develop proctitis after an infection or prolonged stress.
Is a low‑FODMAP diet safe for someone with proctitis?
Yes, as long as you avoid overly restrictive phases during an active proctitis flare. A short‑term low‑FODMAP plan can reduce gas and bloating, which often aggravate rectal pain.
Do I need a colonoscopy if I’ve already been diagnosed with IBS?
If new red‑flag symptoms appear-especially rectal bleeding or sudden weight loss-a colonoscopy is advisable to rule out proctitis or other organic diseases.
What probiotic strains work best for both conditions?
Clinical trials highlight Bifidobacterium infantis 35624 and Lactobacillus plantarum 299v as effective in reducing IBS pain and restoring mucosal integrity in proctitis.
Can stress‑relief techniques replace medication?
Stress‑management alone rarely eliminates severe inflammation, but for many patients it trims down the frequency of IBS flare‑ups and supports healing in mild proctitis when combined with medical therapy.


11 Comments
If you think a quick diet fix solves everything, you’re dreaming.
Most folks read a chart and act like they’re doctors, but they ignore the real inflammation.
Stop treating IBS like a weekend hobby, it’s not that simple.
Dont pretend you know the whole picture, definatly get a proper workup.
Wow, this breakdown is super helpful and super clear!
I love how you highlighted the overlapping symptoms while still showing where they split – it makes the whole thing way less scary.
Keep sharing these gold‑standard guides, because they seriously empower people dealing with gut drama.
Yo this is wild – proctitis and IBS like twins?
Gut drama level 100!
While the enthusiasm is commendable, the prose suffers from a lack of syntactical precision.
The omission of serial commas and inconsistent capitalization distracts from the otherwise valuable content.
A more rigorous editorial eye would elevate the manuscript considerably.
For anyone juggling both, try a low‑FODMAP run for two weeks while keeping a low‑residue diet during flare‑ups – it often eases both the inflammation and the motility issues.
Track your stools with the Bristol chart to see which foods truly trigger you.
It is a tragic irony that modern medicine, for all its technological marvels, still leaves patients wandering through a labyrinth of overlapping diagnoses, clutching pamphlets that only skim the surface of their lived reality.
When a person experiences the gnawing urgency of proctitis, they are often dismissed as merely “IBS‑prone,” a reductive label that betrays a profound lack of empathy.
The gut, a sovereign organ, does not submit to such casual categorization without exacting a toll of frustration and despair.
Moreover, the psychosomatic interplay that fuels stress‑induced motility disturbances cannot be relegated to a footnote in a clinical algorithm.
The literature continues to emphasize statistical significance while ignoring the qualitative nuance of each patient’s narrative.
One must therefore interrogate the epistemological foundations of our diagnostic criteria, lest we perpetuate a system that privileges convenience over compassion.
The pervasive reliance on Rome IV criteria, though undeniably useful, should be complemented by a holistic assessment that includes dietary patterns, psychosocial stressors, and microbial diversity.
In practice, clinicians who adopt a purely reductionist stance risk alienating those who most need a compassionate ear and a flexible therapeutic plan.
The therapeutic overlap-probiotics, low‑FODMAP regimens, and mindfulness-is a testament to the interconnectedness of these disorders, yet guidelines often present them as mutually exclusive pathways.
This dichotomy is not only intellectually dishonest but also clinically dangerous, as it may delay appropriate anti‑inflammatory treatment for proctitis.
Patients report that a simple act of acknowledging their pain as “real” can dramatically improve adherence to treatment regimens.
Likewise, the incorporation of pelvic floor biofeedback, when indicated, demonstrates the merit of interdisciplinary collaboration.
It would be remiss not to mention that socioeconomic barriers further compound the difficulty of obtaining colonoscopic evaluation, thereby widening health disparities.
Ultimately, the onus lies upon the medical community to transcend the sterile language of textbooks and engage with the messy, human experience of gut disease.
Only then can we hope to transform the current paradigm from one of mere symptom management to one of genuine healing.
Oh great, another “miracle” chart that tells you everything about your gut 🚀😂
If only life were as simple as matching symptoms on a webpage, we’d all be cured by now.
Thanks for the groundbreaking insight, truly.
Looks decent but could use more depth.
I notice many people overlook how chronic stress silently fuels both inflammation and motility issues, creating a feedback loop that worsens symptoms.
The subtle interplay between psychological factors and physical manifestations deserves more attention.
This guide hits all the right notes – clear, practical, and hopeful!
Feeling less alone in this journey is priceless, and your tips make it doable.
Thanks for sharing such a balanced resource.
Well, isn’t this just the culinary equivalent of a fireworks show in your colon? 🎆🤦♂️
Who needs a simple life when you can have an endless parade of cramping, bloating, and mystery mucus?
Bravo for turning gastroenterology into a circus act, truly a masterpiece of chaos! 🎪💥