
Prescription drug prices is the cost of medications dispensed by pharmacies, which in the U.S. are uniquely decoupled from government price controls found in other developed nations. In most countries, the government simply tells drug companies what they are willing to pay. In the U.S., for the longest time, manufacturers had a nearly blank check.
The Legal Loophole That Blocked Lower Prices
For over two decades, the U.S. government was legally forbidden from fighting for better prices on behalf of its seniors. The Medicare Modernization Act of 2003 is a federal law that created the Medicare Part D prescription drug benefit but specifically prohibited the government from negotiating drug prices directly with manufacturers . Think of it like going to a car dealership but being legally banned from haggling over the price. For twenty years, the government had to pay whatever the pharmaceutical companies asked.
While other OECD countries use reference pricing or direct negotiation to keep costs down, the U.S. allowed manufacturers almost total autonomy. This created a massive incentive for companies to keep prices high because they knew the largest buyer in the world-the U.S. government-couldn't say no. Even with recent changes, this legacy of non-negotiation still haunts the system.
The Hidden Middlemen: Pharmacy Benefit Managers
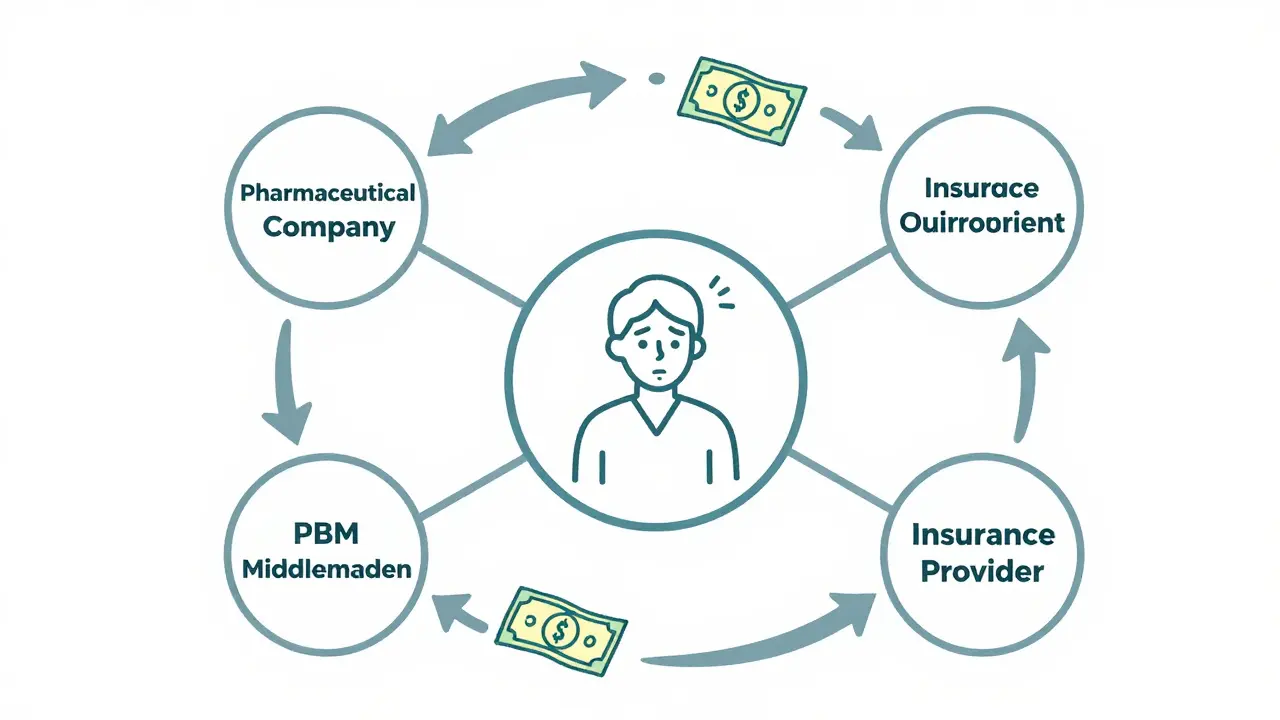
You've probably heard of your insurance provider, but you've likely never heard of the people who actually decide which drugs your insurance covers. Meet the Pharmacy Benefit Managers (or PBMs) which are third-party administrators that manage prescription drug programs for insurers and employers, negotiating rebates with manufacturers . On paper, PBMs should save you money by negotiating discounts. In reality, the system is warped.
PBMs often prefer drugs with higher "list prices" because they get larger rebates from the manufacturer. If a drug costs $1,000 and the PBM gets a $400 rebate, that's a bigger win for the PBM than if the drug just cost $500 to begin with. The patient, meanwhile, often pays a coinsurance percentage based on that inflated $1,000 list price. It's a vertical integration nightmare where the people meant to lower costs actually have a financial incentive to keep the sticker price high.
The Cost of "Innovation" and R&D
Pharmaceutical companies always argue that high prices are necessary to fund research and development (R&D). They claim that without these profits, the next cure for cancer or Alzheimer's would never be discovered. While R&D is expensive, the data often tells a different story. Many of the most profitable drugs are not the result of risky breakthroughs but "evergreening"-making a tiny change to an old drug to get a new patent and keep prices high for another decade.
The recent surge in costs hasn't been driven by rare cures alone, but by novel obesity and diabetes medications. According to the IQVIA Institute, the U.S. market at net prices grew by 11.4% in 2024, largely because of these blockbuster drugs. When a drug becomes a lifestyle necessity for millions, the profit potential becomes astronomical, and prices skyrocket accordingly.
| Feature | United States | Other OECD Nations (e.g., Canada, UK, Germany) |
|---|---|---|
| Government Negotiation | Very limited (Started recently with IRA) | Standard practice for all essential drugs |
| Price Caps/Reference Pricing | Generally none | Strict caps based on similar drugs or international averages |
| Middlemen Influence | High (PBMs drive rebate structures) | Low (Government sets the price) |
| Patient Cost Burden | High out-of-pocket potential | Subsidized or capped by national health systems |
Recent Attempts at Reform: The Inflation Reduction Act
Things are starting to shift, albeit slowly. The Inflation Reduction Act (IRA) is a landmark piece of legislation that finally allows Medicare to negotiate prices for a select number of high-cost drugs and mandates rebates if prices rise faster than inflation . This is the first time the government has been allowed to act as a real buyer in the market.
For example, as of 2025, the IRA established a $2,000 annual out-of-pocket cap for Medicare prescription drug coverage. For someone with a chronic illness, this is a game-changer. However, the reach of these reforms is still limited. By 2026, the negotiation program will only cover ten drugs. While the White House has claimed success in bringing prices for drugs like Ozempic and Wegovy down to around $350 monthly, millions of other medications remain untouched by these rules.

The Reality for Patients: Rationing and Debt
When prices stay high, patients make impossible choices. It's not just about a tighter budget; it's about "medication rationing." This happens when a person splits their pills in half or skips doses entirely because they can't afford the full month's supply. When a drug for a rare disease costs $88,800 a year, any gap in insurance or a change in plan can lead to immediate financial ruin.
Specialty drugs-those used for cancer or endocrine conditions-are the biggest drivers of this crisis. They aren't generic; they are proprietary, and the companies hold the patents. This gives them a legal monopoly. If you need a specific biologic drug to survive and there is no generic version available, you pay whatever the manufacturer demands. This is why the U.S. spends so much more on health per capita than any other nation, yet often sees worse health outcomes in chronic disease management.
Why don't we just use generic drugs for everything?
Generics are great, but they only exist after a patent expires. Pharmaceutical companies use a tactic called "evergreening," where they make slight modifications to a drug's formula or delivery method to secure a new patent, effectively blocking cheaper generics from entering the market for years.
Do PBMs actually help lower costs?
In theory, yes. In practice, their vertical integration with insurers and pharmacies often creates a conflict of interest. They may favor higher-priced drugs because they receive larger rebates from manufacturers, which benefits the PBM's bottom line more than a lower list price would benefit the patient.
Does the Inflation Reduction Act actually work?
It's a start. The $2,000 out-of-pocket cap for Medicare beneficiaries is a major win. However, it only affects a small number of drugs through direct negotiation, and critics argue that subsequent budget bills have weakened some of its most effective provisions.
Why can't the U.S. just adopt the UK's pricing model?
The UK has a centralized system (the NHS) that can negotiate as a single entity for the entire population. The U.S. has a fragmented system of private insurers, Medicare, and Medicaid, which makes a single national price much harder to implement without significant legislative overhaul.
Will drug prices ever actually go down?
It depends on policy. Direct government negotiation and the removal of patent loopholes are the most effective ways to drop prices. While some progress has been made with the IRA, systemic change requires addressing the role of PBMs and the lack of international reference pricing.
What to Do If You Can't Afford Your Medication
If you're struggling with costs, don't just stop taking your meds. There are a few practical steps you can take. First, ask your doctor for a therapeutic alternative-a different drug in the same class that might be cheaper or available as a generic. Second, look into Patient Assistance Programs (PAPs) offered by the manufacturers themselves; these can sometimes provide drugs for free or at a deep discount for low-income patients.
Finally, use price transparency tools. Since the HHS is pushing for more real-time pricing information, use apps or websites that compare pharmacy prices in your area. The difference between two pharmacies just a few blocks apart can sometimes be hundreds of dollars for the same prescription.


14 Comments
It is really great to see more people talking about the IRA and the $2,000 cap. It's a solid step in the right direction and could genuinely save lives for a lot of folks out there.
Typical globist nonsense. We pay the premium because we're the only ones actually funding the R&D that saves the rest of the world's sorry hides! 🇺🇸 Without US capital, you'd all be praying to leeches for a cure. It's called the cost of leadership, deal with it! :-)
Actually, the R&D argument is a total fairy tale 🙄. Most of these companies spend more on marketing and stock buybacks than they ever do on actual lab work. It's morally bankrupt to hold patients hostage for 'innovation' when they're just tweaking a molecule to keep a patent alive 🤡. Absolute scam!
One must wonder if the perceived 'failure' of the system is actually a carefully orchestrated facade designed by the globalist elite to keep the American populace in a state of perpetual medical dependency. It is quite amusing how the masses cling to the notion that legislation like the IRA is a genuine cure, rather than a mere palliative measure to prevent a full-scale revolt against the pharmaceutical industrial complex. I find it rather quaint that we believe the PBMs are simply 'middlemen' and not agents of a much deeper, more sinister financial architecture. The reality is likely far more clandestine than a few loopholes in the 2003 Act. Truly, the ignorance is breathtaking. 😊
pbm just taking cuts while people suffer
This whole post is just basic. Everyone knows about PBMs. Why act like this is some big reveal? It's just a lazy summary of things we've known for years. Maybe try finding something actually new instead of regurgitating a Wikipedia page for us.
I think it might be helpful for some of us to look at the PBM issue from a more systemic perspective. It's a complex web, but understanding it helps us all navigate the system better.
Honestly, it is absolutely tragic that we live in a society where the 'wellness' of a person is measured by the profit margin of a corporation, and frankly, the way people just accept this as 'the way things are' makes me physically ill because the spiritual bankruptcy of the American healthcare system is far more devastating than any physical ailment these overpriced pills are supposed to treat, and yet we continue to dance around the truth while the corporate overlords feast on the desperation of the sick and the dying in a cycle of greed that would make a medieval landlord blush with shame!
Its just wild how we treat health like a bizness instead of a human right!! we gotta vibeee with a new way of thinkin' where love and care come before the dollar sign. lets just imagine a world where we all just look out for each other without these greedy suits in the way!! ✨🌈
The vertical integration of the PBM ecosystem is fundamentally skewed!!! The rebate arbitrage mechanisms are absolutely egregious!!!! We are seeing a systemic failure in the fiduciary duty to the patient-consumer!!!!
While the fragmented nature of the US market is a significant hurdle, there is a profound ethical tension here between intellectual property rights and the universal right to health. The use of 'evergreening' is particularly concerning from a bioethical standpoint, as it prioritizes rent-seeking over genuine therapeutic advancement. We should strive for a middle ground where innovation is incentivized through prizes or public funding rather than through exclusionary patents that price out the vulnerable.
FIGHT THE SYSTEM!!! DEMAND BETTER!!! WE CAN CHANGE THIS!!!!
Omg this is so heartbreaking!! :'( I can't even imagine having to split pills just to survive! We need more awareness on this immediately!! Who is actually fighting for the people?? :O
I appreciate the practical tips at the end. Using transparency tools can really make a difference for people who are struggling right now.